
Legal Blog

Operation Brace Yourself: A Look at the Data
Operation Brace Yourself, the Department of Justice’s 2019 effort to combat massive fraud in terms of durable medical equipment, has gotten a lot of attention and generated many press releases, but I thought it would be useful to look closer at the underlying Medicare data, something that I’ve done extensively in prosecuting and defending health care fraud cases. This will help show the problem that the government tried to address and some issues that attorneys and healthcare professionals should consider.
Operation Brace Yourself, the Department of Justice’s 2019 effort to combat massive fraud in durable medical equipment, has gotten much attention and generated many press releases. Still, I thought it would be helpful to look at the underlying Medicare data, which I’ve extensively done in prosecuting and defending health care fraud cases. This will help show the problem that the government tried to address and some issues that attorneys and healthcare professionals should consider.
First, Operation Brace Yourself was a response to a problem that grew to staggering amounts over several years.
According to my review of Medicare data, no doctors or medical professionals anywhere in the country ordered huge amounts of prosthetics or orthotics (at least $1 million) until 2015. That year, for the first time, two providers each ordered more than $1 million of POS—I’ll call them “high-volume POS referrers.”
This was unusual. One of these high-volume POS referrers treated less than 200 Medicare beneficiaries that year while ordering POS for more than 1,500. In other words, he was ordering POS for hundreds of patients whom he probably had never even seen or treated.
And the number of such high-volume POS referrers went up year after year. By 2018, about 170 Medicare providers ordered more than $1 million of POS that year, with about 24 ordering more than $5 million each (including one doctor who ordered more than $15 million), according to billing data.

This was a huge change in billing patterns—a very concentrated amount of POS orders from physicians who often had not ordered much in POS beforehand. Some of these physicians were in specialties that ordinarily would not be associated with ordering large amounts of expensive back braces and knee braces.
There were many family practitioners, many nurse practitioners, some OB-GYNs, an ENT (ear, nose, and throat doctor), and even a psychologist and a psychiatrist. Many of these doctors and practitioners ordered braces for thousands of patients (based on data submitted by DME suppliers) while actually treating a much smaller number of patients (based on the Part B data submitted by the doctors and practitioners themselves).

These are massive red flags in the data, and the Operation Brace Yourself cases explain what was going on. As we now know from the publicly filed documents, many of these doctors participated in schemes involving “telemedicine.” However, “telemedicine” here was unlike the virtual visits many of us used because of the pandemic.
In everyday situations involving DME, the doctor treats the patients and orders DME as part of the patients’ overall care. But here, the doctor was not the primary decision-maker, often had no prior relationship with the patients, and often had little if any interaction with the patients - sometimes just a telephone call. In the cases that the government calls “telemedicine” cases, businesspeople and marketers are the main drivers of the process, and doctors often sign off on expensive orders based on minimal patient information and often without fully understanding what is going on.
The diagram below shows how a prosthetics order should work in normal circumstances. A patient goes to a doctor, the doctor places an order to a supplier, and the supplier bills Medicare for the DME that the patient receives and uses.

The following diagram shows how prosthetics orders in the Brace Yourself cases came about. According to the claims submitted to Medicare, everything worked as usual.
But in reality, patients were recruited by call centers, a doctor who had little to no interaction with a patient signed orders for braces, and a broker sold the patient information and those signed orders to suppliers who then billed Medicare for expensive items that patients often did not need or even use.
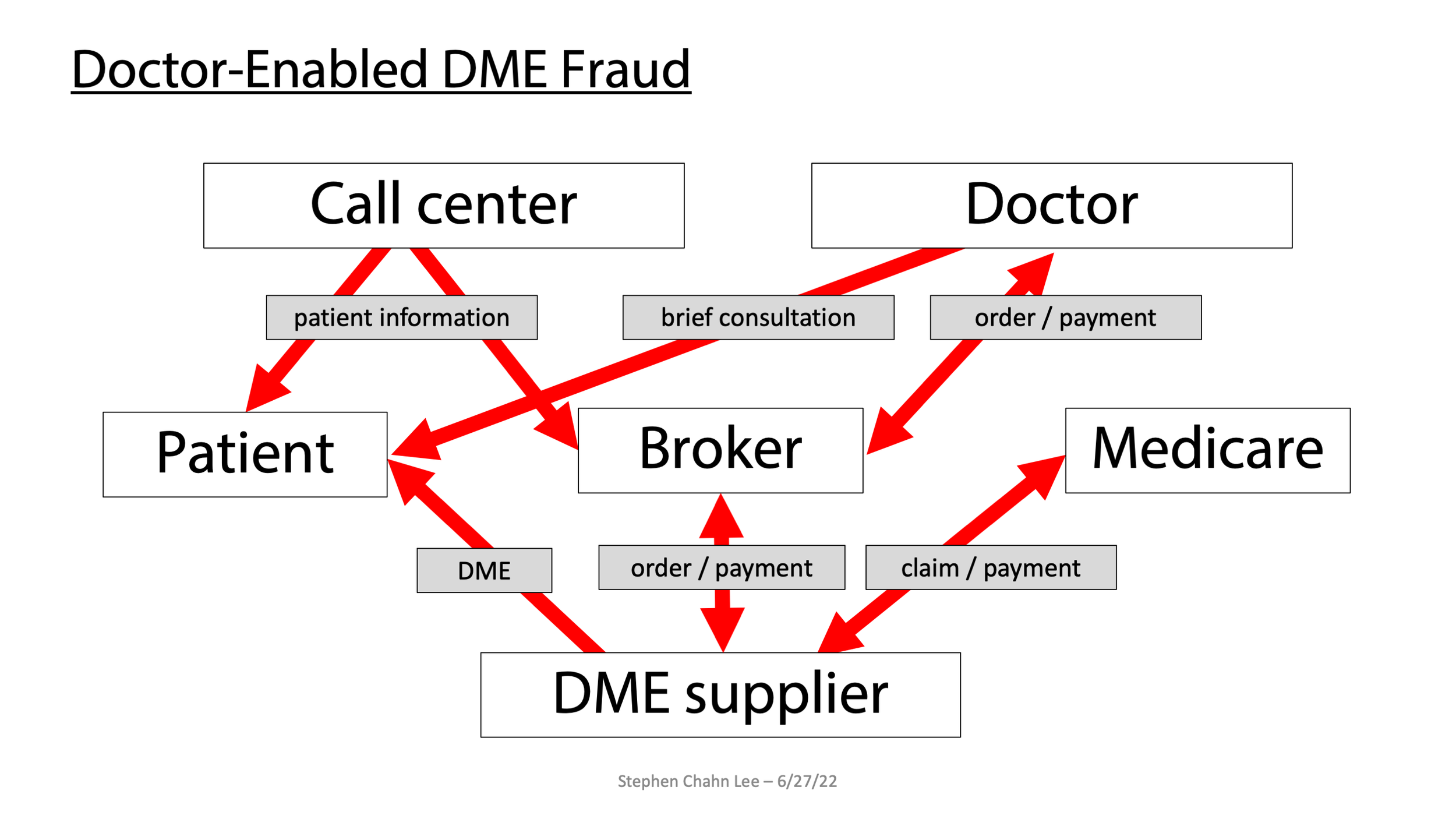
Overall, this is a complex system set up to defraud Medicare by billing for unnecessary items in ways that appear legitimate.
Many of these cases involve some telephone contact with a doctor. Still, it’s more beneficial to consider these cases as “doctor-enabled” healthcare fraud, in contrast to classic healthcare fraud schemes where the doctor drives the fraud. Based on my experience, what the government calls “telemedicine” fraud is just a slight evolution of similar schemes in other areas such as home health, hospice, and genetic testing – all cases where the doctor enables the fraud rather than driving the fraud. “Telemedicine” focuses on one delivery system rather than the more significant problem.
Whatever you call it, all of this had enormous consequences on Medicare.
In 2018 alone, Medicare spent almost $500 million on POS ordered by these high-volume POS referrers. From 2015 to 2019, Medicare paid over $1.1 billion on POS allegedly ordered by these people.

Second, Operation Brace Yourself does appear to have had a significant impact on the problem.
The government charged and arrested multiple people in April 2019, and the charges appear to explain a significant drop-off in activity over the entire year. The number of providers responsible for more than $1 million of POS dropped, and Medicare spending on POS for those high-volume referrers dropped by about 30 percent. I’ve heard one government official say there was a $2 billion decrease in spending in the 18 months after Operation Brace Yourself, a sign of how big the problem had gotten and how much it would have cost Medicare had the problem continued.
Third, the government has charged and convicted several doctors who ordered large amounts of POS.
According to Medicare data, as of June 2022, several doctors who have been charged and convicted are listed below, along with the amounts of POS they ordered.
Dr. Kenneth Pelehac was charged in 2022, pled, and agreed to cooperate, but has not yet been sentenced—total Medicare POS payments of more than $17 million.
Dr. Ravi Murali - charged in 2020, pled and sentenced to 54 months imprisonment—total Medicare POS payments of more than $13 million.
Dr. Randy Swackhammer - began cooperating with the government in early 2019 (while Operation Brace Yourself was still a covert operation) and made recordings of others. Charged in 2019, pled, cooperated, and sentenced to probation—total Medicare POS payments of over $7 million.
At least two high-volume referrers who were charged are set for trial in late 2022.
At the same time, as of June 2022, most high-volume referrers, including some doctors with very high POS payments associated with them, have not been charged.
For example, according to data, the doctor who ordered the most POS ($24 million in total, including a staggering $17 million in just 2019 alone) has not been charged with a crime as of June 2022. According to data, she treated about 400 patients in 2019 while ordering POS for thousands of patients she never treated – more than 8,000. I assume the government has looked at this doctor, who probably got involved with “telemedicine” because she was in bad shape financially - she filed for bankruptcy in early 2019 and mentioned her work in “telemedicine” in her bankruptcy petition. Whether she gets charged will probably depend on whether the government can prove that she knew that her conduct was illegal.
Fourth, these doctors appear to have made relatively little from their involvement compared to the DME suppliers.
According to publicly filed documents, several doctors who have been charged made $20 to $40 per order they signed. In one example, the doctor made $30 for authorizing a knee brace for a patient he had never met or spoken to, while the DME company was paid more than $300 for that brace. Plea agreements with two doctors show that the doctors made less than $200,000 each for their parts in the overall crime, while Medicare paid millions of dollars to the DME suppliers who used the doctors’ orders.
In contrast to some of these doctors, some patient brokers and DME suppliers who have been charged and convicted as part of Operation Brace Yourself reportedly made far more money. In one case, two people were sentenced to more than 12 years in prison for a scheme that allegedly resulted in more than $27 million of Medicare payments, including millions that the defendants transferred overseas. Another man was sentenced to 15 years in prison for selling patient information; he notably engaged in this conduct before Operation Brace Yourself and continued the conduct even afterward.
So what can attorneys and health care providers take from all this?
First, there is a lot of data out there, both publicly and privately, and people should get a better handle on the data sooner rather than later. Many of the high-volume referrers probably had no idea how much money was being spent under their name and how easily the data pointed to them, and they probably would have withdrawn quickly. They could have avoided prosecution if they had known. Some of these doctors might have been the victims of identity theft, and a closer look at their data might have caught that, too.
If a doctor has already been charged, it may be helpful to know how the doctor compares to his or her peers. Such comparative data may help position the doctor better, at least for sentencing, especially when it is clear that many people have not been charged for what seems like similar conduct.
Second, many doctors who ordered large amounts of POS were in fields not generally associated with prosthetics or orthotics. Some of these doctors probably thought this work was a way to supplement their income without realizing the massive risks they were taking by getting involved in unfamiliar areas. Doctors should be careful when switching fields or going outside their specialties and not just rely on what their employers tell them.
Third, the government has to prove “willfulness” to prosecute someone for health care fraud or kickbacks – basically, the government has to prove that people knew that what they were doing was illegal and did it anyway. That can be difficult when the doctors have little knowledge of the overall system and receive relatively small payments. If a doctor were naïve, careless, or gullible, the doctor would not have the “willfulness” necessary to be convicted of healthcare fraud. This might explain why many high-volume referrers have not been charged with a crime.
At the same time, the government can prove willfulness more easily when fake documents are used, such as when businesspeople or DME suppliers try to make payments to doctors look like “marketing” expenses, indicating that they know that the payments violate the Anti-Kickback Statute.
Doctors involved with DME or other high-risk areas can alert themselves to potential “doctor-enabled” healthcare fraud by asking a few questions.
Do you know where your patients came from? Are your patients reaching out for help, or have marketers solicited them?
Are you treating the patient or just ordering one or more particular items or services that you would not order in your typical practice?
Is everything true before you sign if you are given forms or EMRs to fill out? If not, this could be a red flag for fraud.
How are you getting paid? Are your services being billed to a patient’s insurance, or are they effectively tied to your ordering another service or item? If the latter, your payments could be seen more like a kickback.
The Stephen Lee Law legal blog covers various topics, including healthcare fraud defense, investigations, data analytics, and the federal anti-kickback statute.
For further insights into Operation Brace Yourself or legal guidance on healthcare fraud defense, please contact Stephen Lee Law.

Willfulness: Often-Overlooked in Healthcare Fraud and Kickback Cases
When it comes to healthcare fraud and kickback cases, I believe many attorneys – both prosecutors and defense attorneys – overlook one important element – “willfulness.” There are four main federal criminal statutes covering healthcare fraud (18 U.S.C. 1347, the Anti-Kickback Statute, false statements, and obstruction). All of them require the government to prove beyond a reasonable doubt that the defendant acted “willfully.”
Regarding healthcare fraud and kickback cases, I believe many attorneys – both prosecutors and defense attorneys – overlook one crucial element – “willfulness.”
Four main federal criminal statutes cover healthcare fraud (18 U.S.C. 1347, the Anti-Kickback Statute, false statements, and obstruction). All of them require t e government to prove beyond a reasonable doubt that the defendant acted “willfully.”
Understanding 'Willfulness' in Healthcare Fraud
Willfulness is the critical element that distinguishes a criminal case from a case that should be handled civilly or administratively. Prosecutors and law- forcement agents often take this element for granted, but attorneys and practitioners should examine this element more closely.

Willfulness: The Defining Criterion
So what does it mean to act “willfully”?
Five circuits define “willfully” in their pattern jury instructions in the same way that the government has to prove beyond a reasonable doubt that the defendant knew what he or she was doing was illegal.
1st Circuit: “An act or failure to act is ‘willful’ if done voluntarily and intentionally, and with the specific intent to do something the law forbids, or with the specific intent to fail to do something the law requires to be done; that is to say, with bad purpose either to disobey or to disregard the law.” Instruction 4.18.1347 (healthcare fraud).
3rd Circuit: “That [defendant] knew [his/her] conduct was unlawful and intended to do something that the law forbids. That is, to find that [defendant] acted willfully, you must find that the evidence proved beyond a reasonable doubt that [defendant] acted with a purpose to disobey or disregard the law.” Instruction 5.05 (note that the 3rd Circuit does not explicitly include “willfully” in its healthcare fraud instruction – make sure to ask for this to be included!).
5th Circuit: “[T]he act was committed voluntarily and purposefully, with the specific intent to do something that the law forbids; that is, to say, with bad purpose either to disobey or disregard the law.” Instruction 2.59 (healthcare fraud).
8th Circuit: “A defendant acts willfully if he knew his conduct was wrongful or unlawful.” Instruction 6.42.1320 (note that this definition is included in the instruction for Anti-Kickback Statute violations but not in the definition for healthcare fraud cases – make sure to ask for this definition to be included in all types of HCF cases!).
11th Circuit: “The act was committed voluntarily and purposely, with the intent to do something the law forbids; that is, with the bad purpose of disobeying or disregarding the law.” Instruction B9.1A (note that the 11th Circuit did not specifically include “willfully in its healthcare fraud instruction – make sure to ask for this to be included!).
The Legal Interpretation of 'Willfully'
Two other circuits have language in their pattern jury instructions suggesting similar instructions:
The Seventh Circuit’s pattern jury instructions for healthcare fraud do not define “willfully” but notes that one 2008 case suggests that “willfully” requires proof that a defendant knows that his or her conduct was “in some way unlawful.” In the cases I handled as a prosecutor in Chicago, we included a version of that definition.
The Ninth Circuit’s jury instructions for healthcare fraud and the Anti-Kickback Statute refer to willfulness, and the notes for Instruction 5.5 state that willfulness in healthcare fraud cases generally requires knowledge that a defendant’s conduct was unlawful.
Following these circuits, willfulness means more than unethical, immoral, or sketchy. While the government does not have to prove that an individual knows the particular statutes that he or she violated, the government has to prove that the individual knew that their conduct violated some law.
Please note that the Sixth Circuit does NOT define willfully the same way as other circuits. In its healthcare fraud instruction (10.05), the Sixth Circuit defines “knowingly and willfully” as follows: “An act is done ‘knowingly and willfully’ if it is done voluntarily and intentionally, and not because of mistake or some other innocent reason.”
The Sixth Circuit’s instruction is, I believe, incorrect as it treats “willfully” as synonymous with “knowingly.” It also appears to not take into account an important case on this topic – United States v. Ajoku (08-1094 in the Central District of California, 11-50230 in the Ninth Circuit, and 13-7264 before the Supreme Court).
In 2011, Kelechi Ajoku, a licensed vocational nurse, was convicted by a jury of making false statements in a healthcare matter under 18 U.S.C. 1035. Defense counsel had asked that willfulness be defined as requiring proof that the defendant “acted with knowledge that his conduct was unlawful.” The district court rejected this request and gave instructions that treated “willfully” as synonymous with “knowingly.”
In 2013, the Ninth Circuit affirmed that instruction. The Ninth Circuit wrote, “[i]n the context of false statement cases … willfulness simply means ‘deliberately and with knowledge,’ and does not require knowledge of unlawfulness.”
The case was appealed to the Supreme Court. 2014, the Solicitor General confessed to the error, and the Supreme Court vacated the judgment.
In 2015, Ajoku was re-tried.
This time, the district court separated “knowingly” and “willfully” in the instructions.
This time, the district court told jurors that the government had to prove that Ajoku had acted “willfully “ with a bad purpose. In other words, the defendant committed the act voluntarily and purposefully, and with knowledge that his conduct was unlawful.”
This time, Ajoku was found not guilty.
Unfortunately, the Sixth Circuit’s jury instruction on healthcare fraud has not been updated in light of the Ajoku case. Some people may have been convicted under this definition and should not have been convicted.
If you’re in the Sixth Circuit, ask for a “willful” definition that fits with other circuits.
Strategic Implications for Legal Practitioners
Regarding evidence, attorneys should look carefully at the facts to determine whether the government can prove willfulness in particular cases. Here are some questions to consider:
Did a defendant sign a Medicare provider enrollment form? If he or she did, the government would use that form as evidence of willfulness because signing that form (1) establishes knowledge of the healthcare fraud statute and the Anti-Kickback Statute and (2) contains the statement: “I will not knowingly present or cause to be presented a false or fraudulent claim for payment by MedicareHowever, But if a defendant did not sign a form, the government may have difficulty proving that he or she acted willfully, particularly when it comes to kickback cases or defendants who are not medical professionals.
What kind of contact did a defendant have with the government before being prosecuted? If a defendant was notified that they were an outlier, that might show willfulness. However, if a defendant was audited and told their claims were acceptable, that might undercut the government’s proof of willfulness.
Does the government’s case relate to something many people get wrong? If so, that could show mistakes and undercut willfulness. For example, office visits and other evaluation and management (E&M) services have a high error rate. In 2010, the government estimated that 55 percent of claims for E&M services were improperly coded and lacked documentation, resulting in $6.7 billion in improper Medicare payments. If so many doctors are making mistakes here, specific evidence in a criminal case should show that it was not just another mistake. Similarly, while cash in unmarked envelopes is an illegal kickback, the further a case gets from that scenario, the harder it will be for the government to show willfulness in a kickback case.
Were there safe harbors that might undercut willfulness even if not technically applicable? There are lots of safe harbors to the Anti-Kickback Statute. If a defendant believed in good faith that he or she fell within a safe harbor, that defendant did not act “willfully” even if he or she was wrong.
What did a particular defendant know or not know? If a defendant was kept in the dark about his or her role, or was misled by his or her employer, or was simply naïve or gullible, that would undercut willfulness. This is especially important in home-health, DME and other “doctor-enabled” fraud cases where doctors often do not understand how the overall fraud is working and may not even understand that they are part of a fraud.
If a defendant talked to the government, did they admit knowing that their conduct was illegal, or did they just acknowledge that there were some erroneous or mistaken claims? The distinction is essential. Admitting in hindsight that a claim was improper is NOT the same as knowing at the time that one’s conduct was illegal.
Prosecutors should scrutinize their cases carefully for evidence of willfulness. If they do not have such evidence, they should consider referring the case for civil or administrative resolution, or they should just decline the case entirely.
Defense attorneys should also scrutinize their call for evidence of willfulness. And if the case has to go to trial, consider focusing the defense on willfulness. Doing so turns the case around by concentrating on a person’s state of mind, an area that the government might have taken for granted and can do little to build up once a case goes over. Focusing a jury’s attention specifically on willfulness might be more effective than trying to defend the legitimacy of particular claims or trying to say that everything had been done perfectly.
The Stephen Lee Law legal blog covers various topics, including healthcare fraud defense, investigations, data analytics, and the federal anti-kickback statute.
For further insights into willfulness or legal guidance with healthcare fraud defense, please contact Stephen Lee Law.